
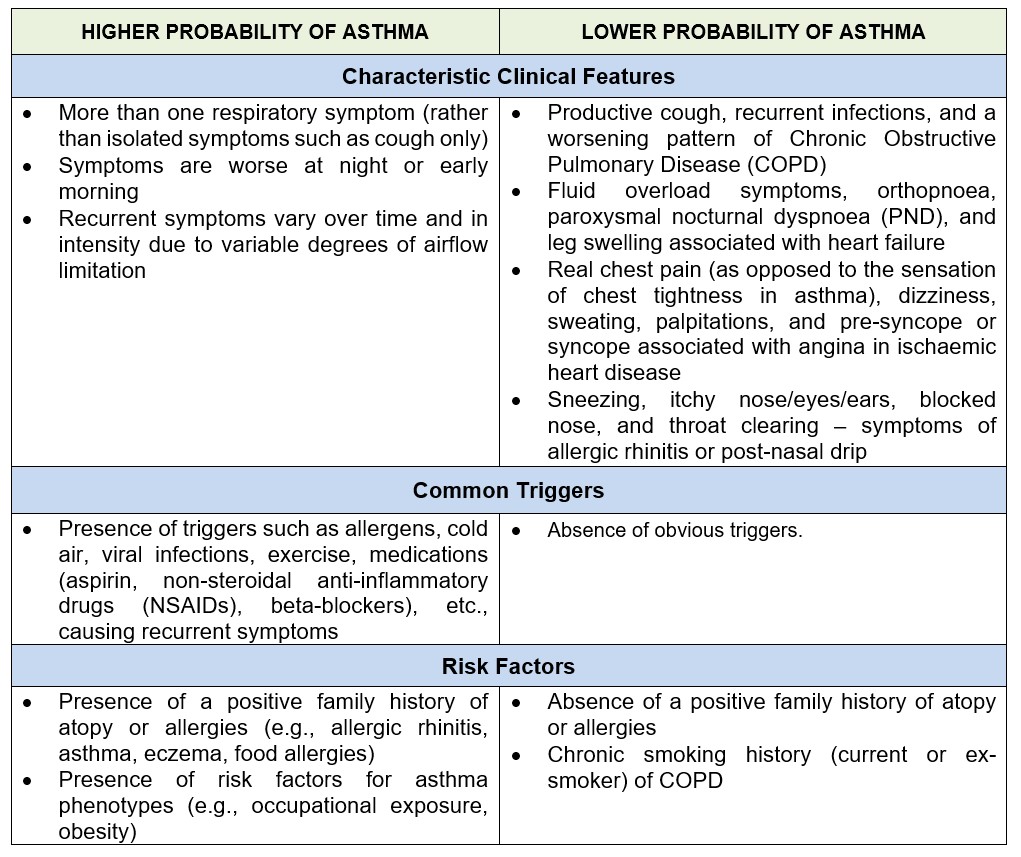
There is no gold standard test to diagnose asthma. The diagnosis of asthma is made based on characteristic history and is supported by positive obstructive airflow variability and reversibility with spirometry. In primary care, besides clinical history, asthma diagnosis has predominantly been made from a trial of medication. Hence, over- and under-diagnosis of asthma are common due to the lack of objective lung function testing to demonstrate variable expiratory airflow limitation.
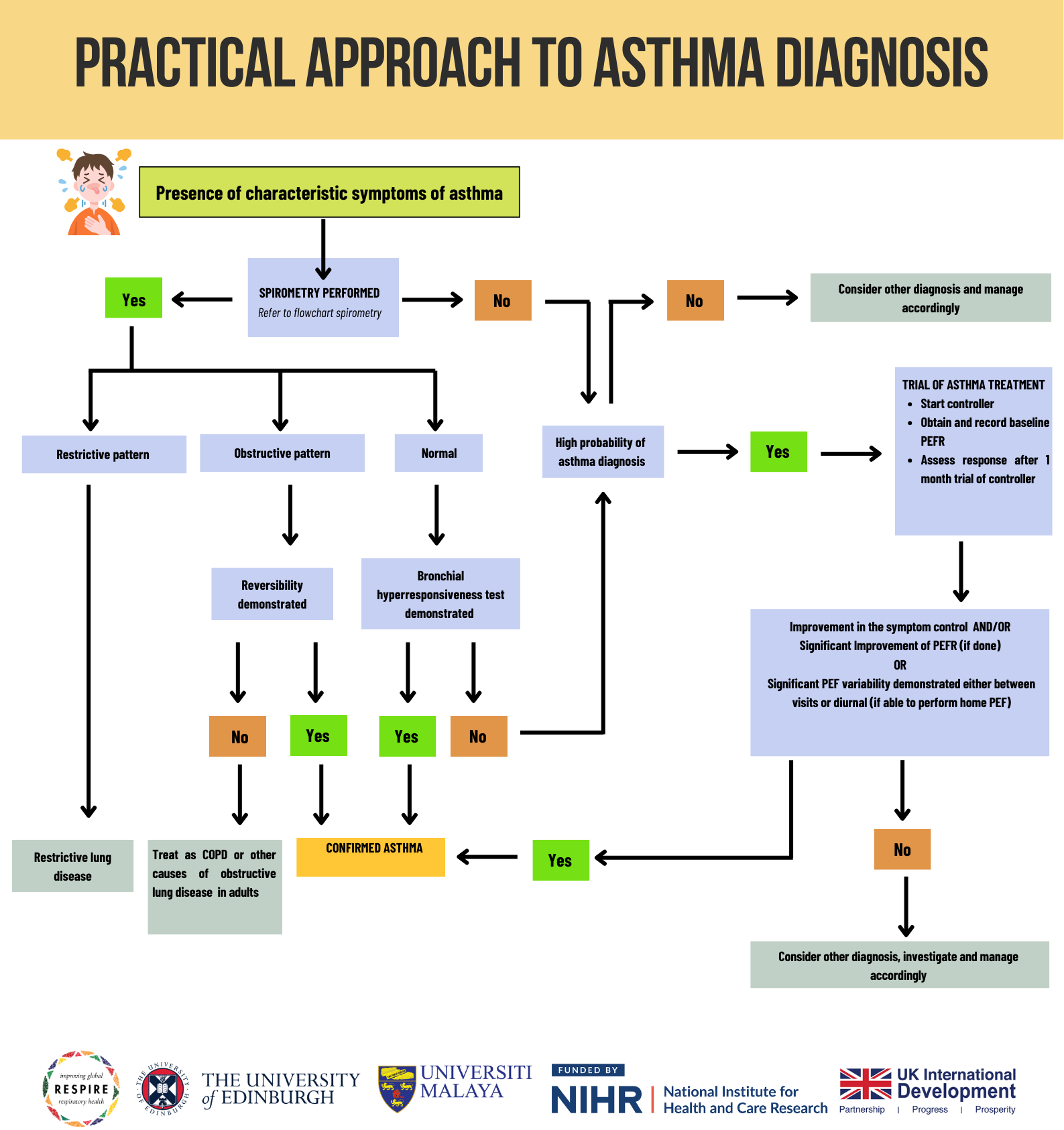
Although spirometry is more reliable for objective measurements of airflow limitation, it is not always available or easily accessible in primary care. Given the resource-limited setting, alternative approaches to diagnosing asthma in primary care are acceptable. Demonstrating excessive airflow variability using peak expiratory flow rate (PEFR) is acceptable with the presence of characteristic symptoms. PEFR is the maximal flow achieved during the maximally forced expiration initiated at full inspiration.
A. Positive bronchodilator reversibility test:
Increase from baseline in PEFR, 10 – 15 minutes after 200 – 400 mcg of salbutamol.
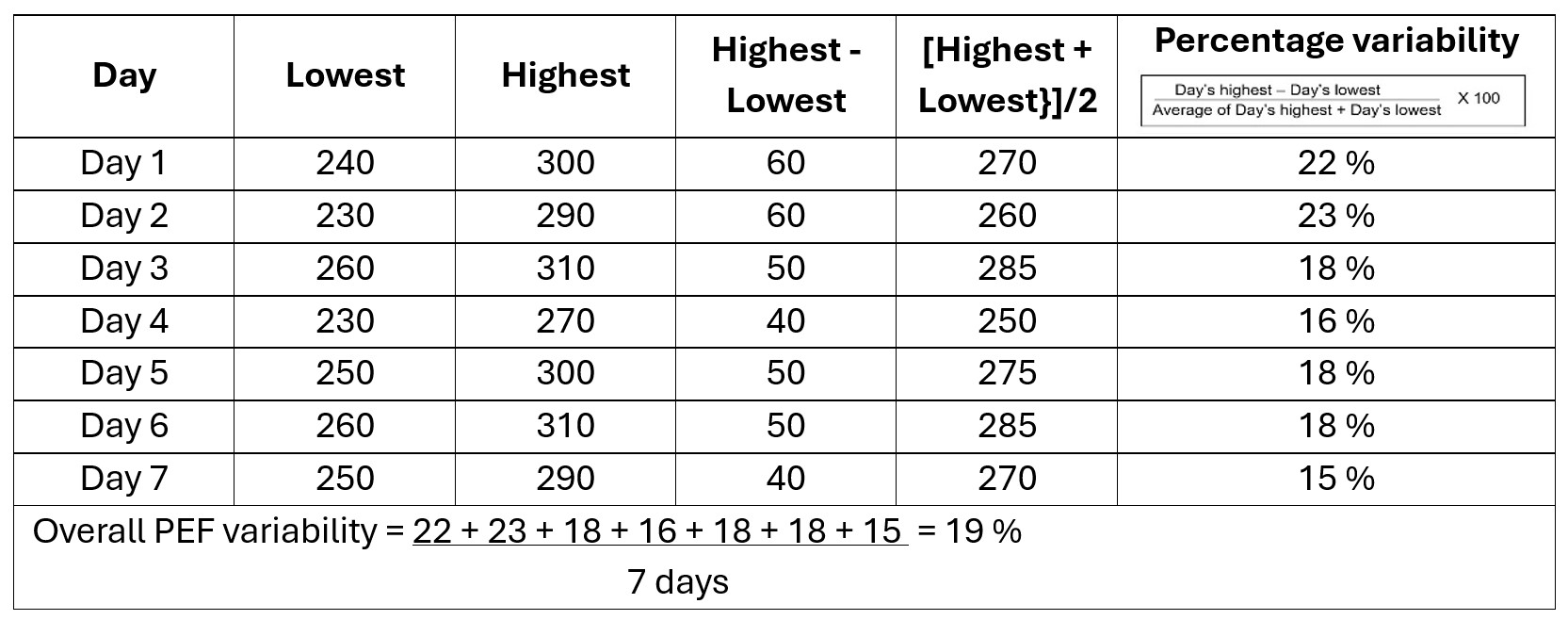
B. Diurnal PEFR variability:

Example of diurnal variability calculation using daily amplitude percent mean method:
C. Significant improvement of PEFR with anti-inflammatory:
With respiratory symptoms characteristic of asthma, a significant improvement by >20% from the baseline after 4 weeks of anti-inflammatory treatment (such as inhaled corticosteroid).
D. PEFR variation between visits:
With respiratory symptoms characteristic of asthma, a change of PEF of at least >20% for adults and >15% for children between visits is accepted.
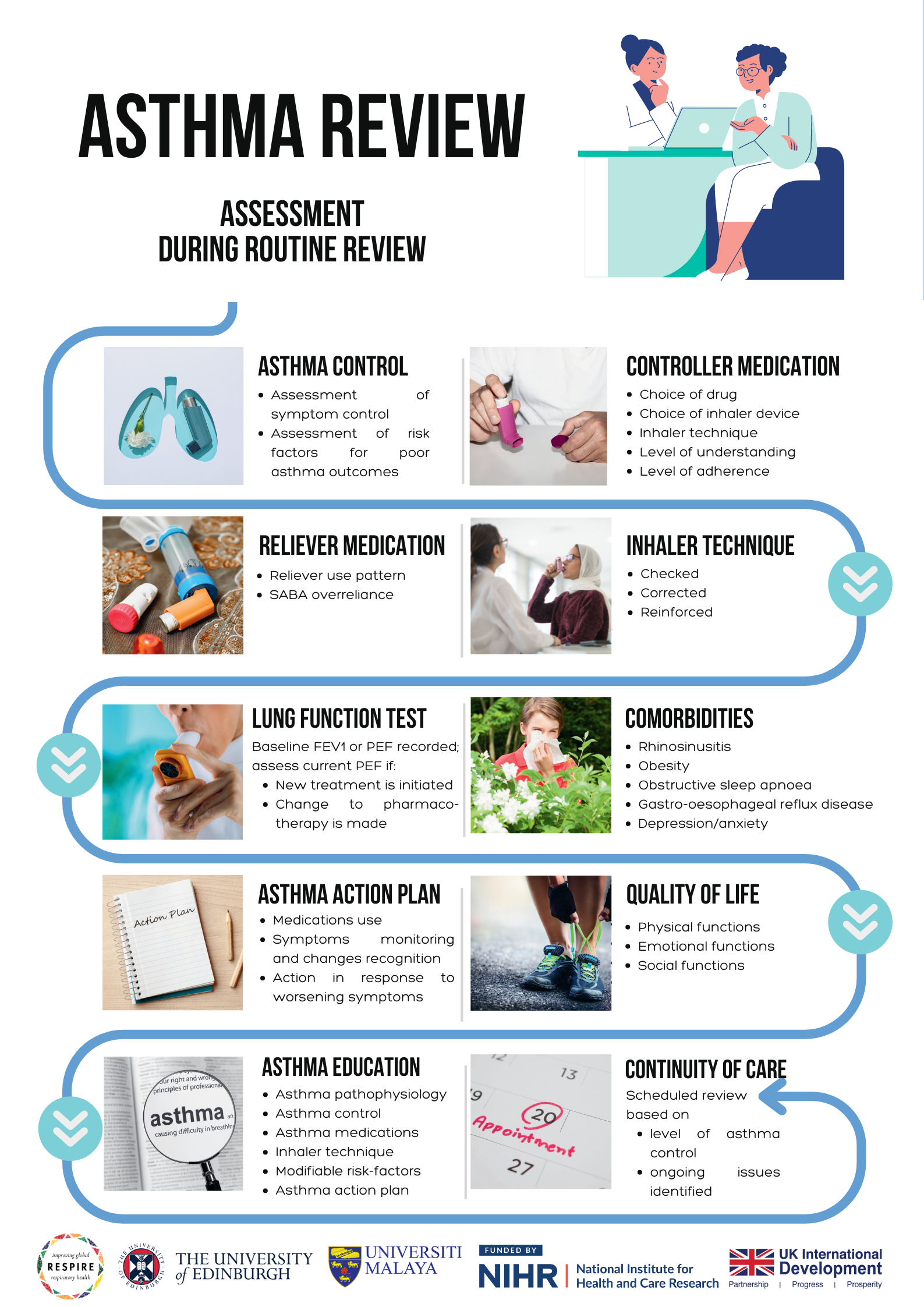
Asthma is a chronic condition that requires ongoing management to ensure symptoms are controlled, quality of life is maintained, and complications are minimised. Regardless of the control level, all patients with asthma should have a regularly scheduled review (follow-up). Individuals with asthma need to adhere to their scheduled appointments for effective monitoring. In an ideal team-based asthma care setting, a comprehensive assessment package could be delivered through collaborative work between team members with appropriate training in asthma, each carrying their own defined roles. A team-based asthma care should include at least doctors, nurses, and pharmacists. However, in a setting with limited human resources and/or a heavy patient load, patients with poorly controlled asthma should be prioritized to receive as comprehensive an assessment and care as possible. Patients with good asthma control should at least receive a basic assessment of care. The routine care for all patients with asthma, performed during each review, should incorporate evidence-based quality indicators. These assessments should also be performed whenever appropriate during the patient’s unscheduled clinic encounters.
Two types of medication are used in the treatment of asthma.
Asthma pharmacotherapy is based on two classes of drugs:
Reliever medications that help to relax and dilate (widen) the narrowed airways resulting in asthma symptoms.
Initiating Pharmacotherapy
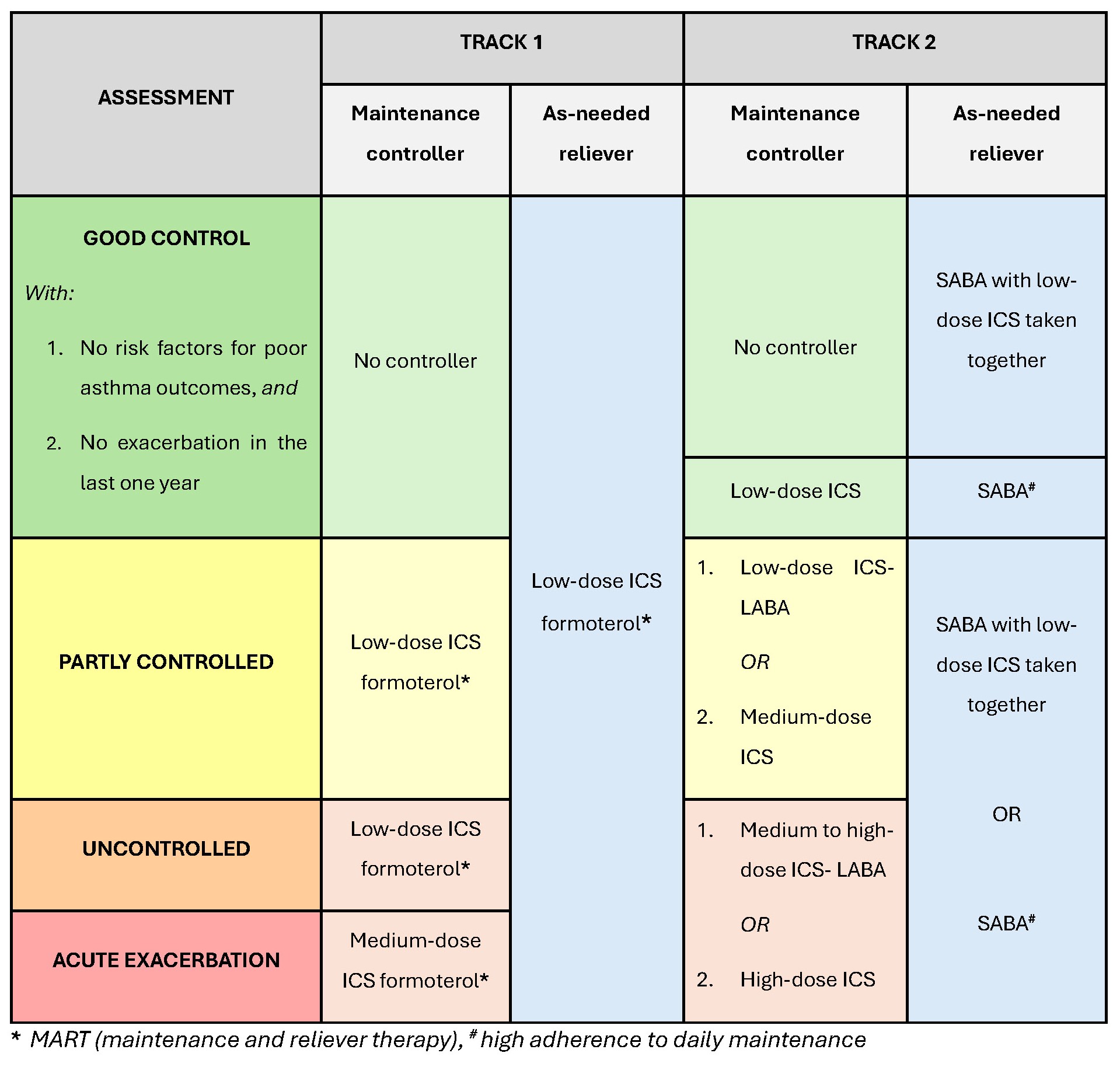
12 years and older
The GINA strategy divides the treatment recommendations for patients 12 years and older into two tracks.
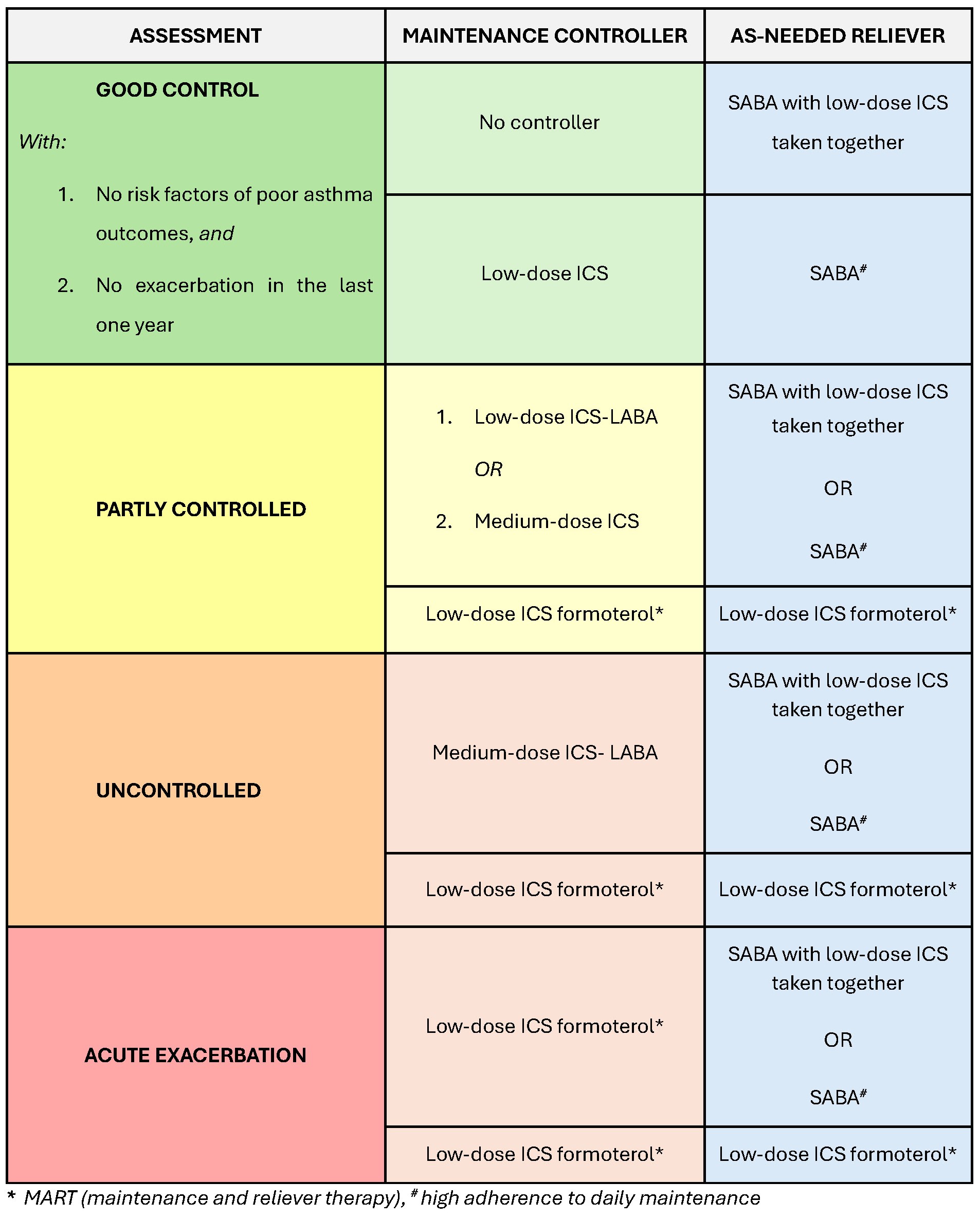
6 – 11 years
The GINA strategy divides the treatment recommendations of patients 6 to 11 years as below.
Optimising Pharmacotherapy
Appropriate adjustment to the treatment regimen may be necessary and should be considered in certain situations such as:
Treatment optimisation can be guided by the GINA 2024 recommendation by step-up and step-down strategies towards the right and the left of the ladder respectively.
Stepping Up the Pharmacotherapy
Stepping Down the Pharmacotherapy
Consider stepping down asthma treatment when a patient:
Asthma management is not just about drug treatment. Non-pharmacological interventions are an important aspect and should be used in combination with medications. If pharmacotherapies are not sufficient to achieve good asthma control, confounding factors such as poor treatment adherence, poor inhaler technique, comorbidities, and exposure to modifiable risk factors should first be ruled out before increasing therapy dosage or resorting to add-on treatments.
The patient's active participation is important in asthma management. All patients should be made aware of the components of asthma self-management, which include:
Refer to the Targeted Asthma Education section for more detail.
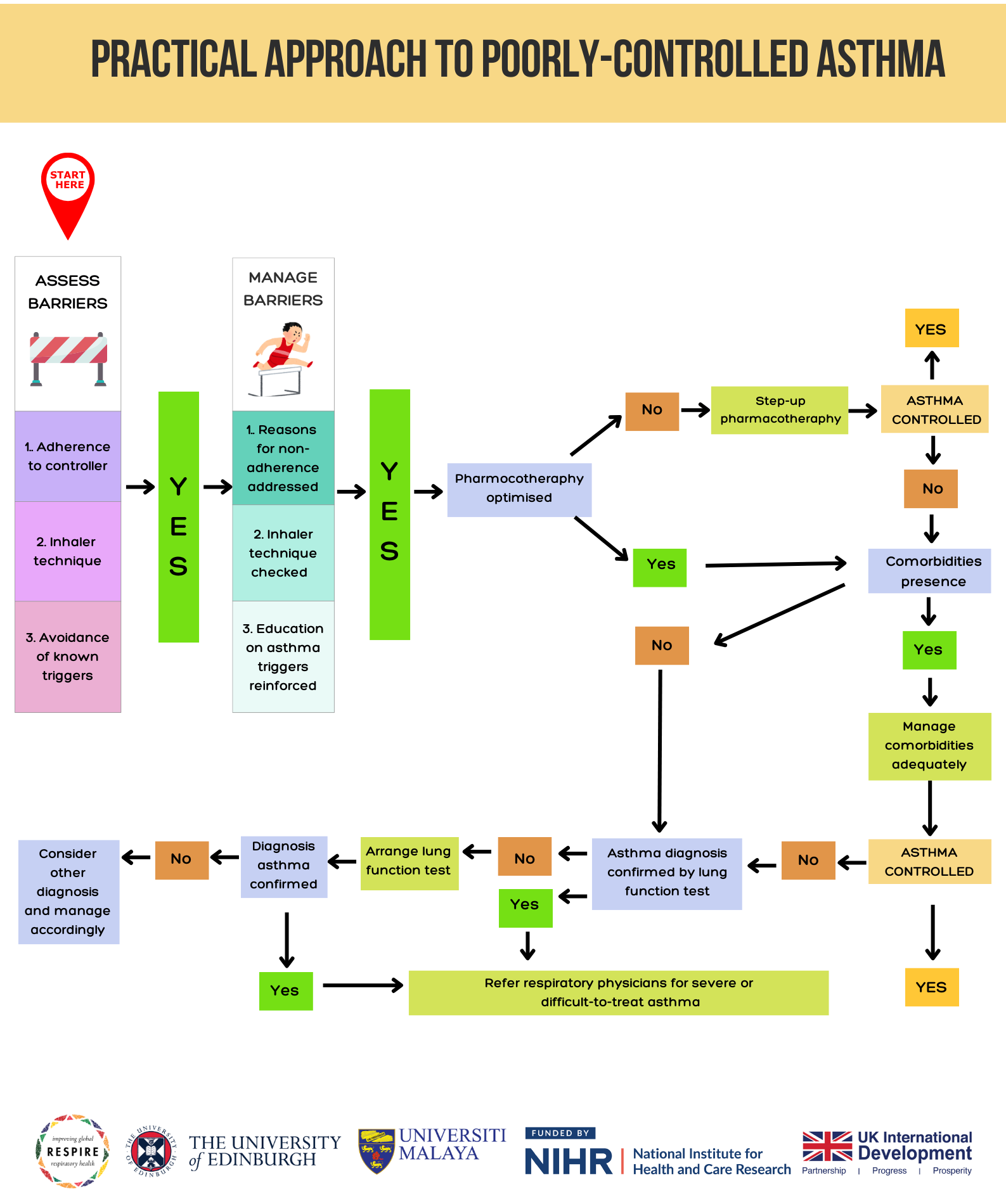
A practical approach to managing poorly controlled asthma involves a systematic evaluation to identify and address underlying issues. Initially, it is crucial to assess and confirm the patient's inhaler technique and adherence to the prescribed treatment regimen. Incorrect use of inhalers and poor adherence are common causes of suboptimal asthma control.
Additionally, identifying and mitigating modifiable risk factors, such as exposure to allergens, tobacco smoke, or environmental pollutants, is essential. Regularly reviewing and updating the patient's asthma action plan can help ensure they are following the appropriate steps during exacerbations. If asthma control remains poor despite these measures, consider stepping up pharmacotherapy according to the Global Initiative for Asthma (GINA) guidelines.
In cases where asthma control is still not achieved, a referral to a specialist for further evaluation and potential treatment adjustment may be necessary. This structured approach helps in pinpointing and resolving factors contributing to poor asthma control, thereby improving patient outcomes.
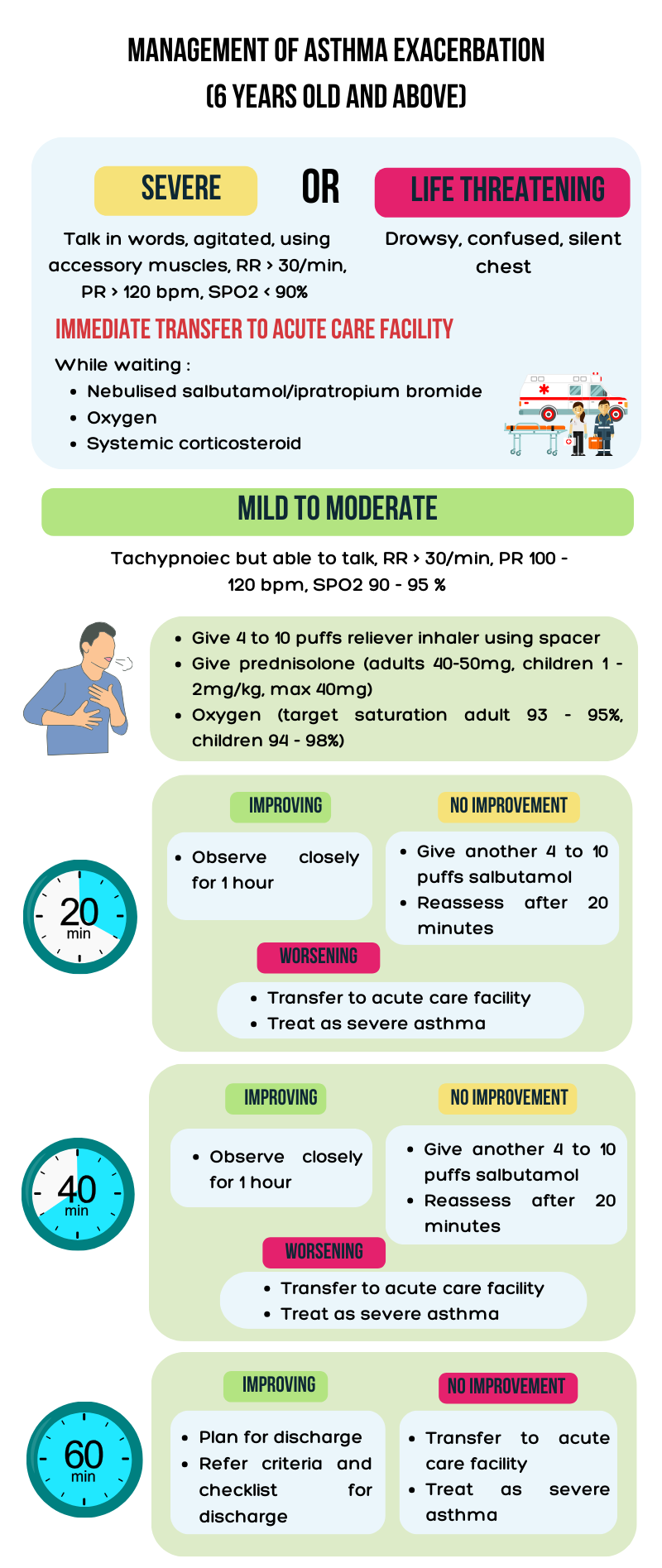
Asthma exacerbation is a progressive decrease in lung function characterised by a progressive increase in symptoms of SOB, cough, wheezing or chest tightness. Asthma exacerbation treatment aims to relieve symptoms and return patients to their best lung function. For most patients, initial treatment with nebulised β-agonist and oral corticosteroids is sufficient. Supplemental oxygen is indicated for hypoxaemia and should be given at a flow rate or concentration sufficient to maintain oxygen saturation > 90%. Hospitalisation is generally required if the patient's condition worsens or fails to improve after optimal treatment for exacerbation has been provided.



Last Update: 25/05/2026